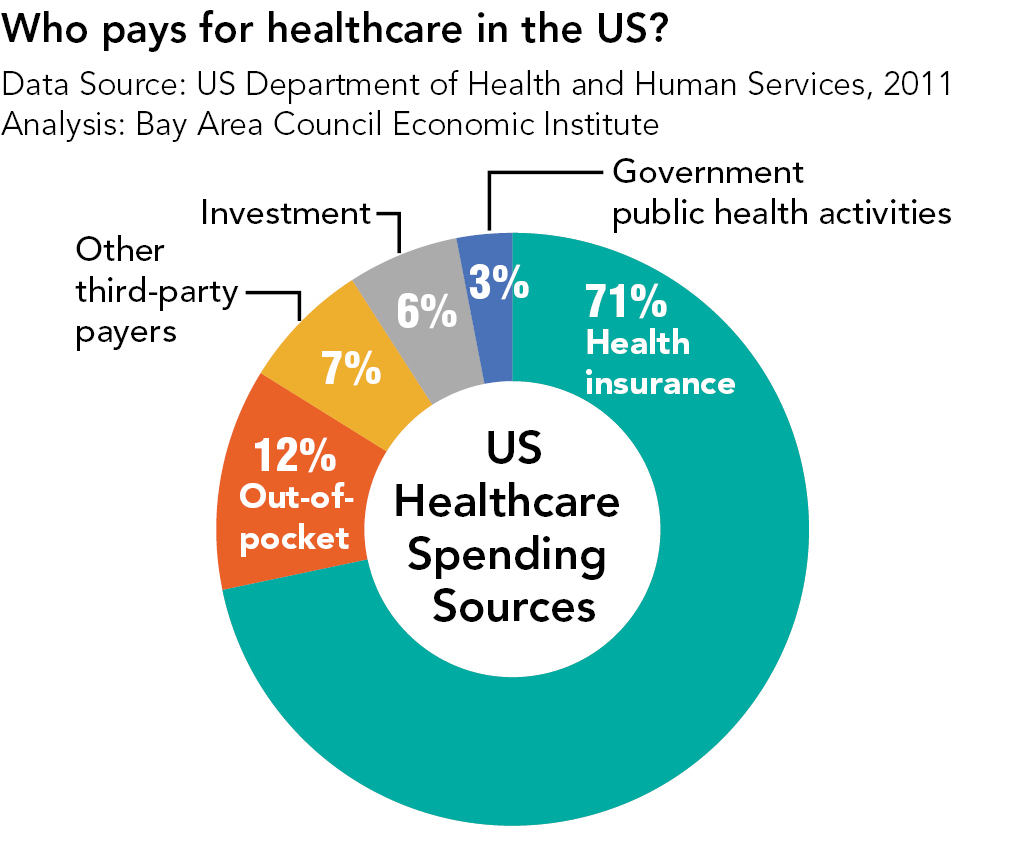
The image presented, ‘Who-Pays-For-Healthcare-In-US.jpg,’ serves as a poignant visual cue, immediately raising questions about the fundamental structures underpinning different systems worldwide. Indeed, the debate surrounding healthcare models globally often culminates in a stark comparison: the US approach, heavily influenced by capitalism, against systems seen elsewhere, particularly as more universal or collectively funded alternatives. Understanding why this divergence exists requires peeling back layers of history, economics, politics, and societal values. Why does the United States predominantly employ a healthcare system structured around private enterprise and market principles, while many other nations view their systems primarily through the lens of social welfare and collective responsibility? This exploration delves into the complex reasons behind this unique landscape.
The Genesis of a Capitalist Framework
Tracing the roots reveals a complex interplay of historical events and prevailing ideologies. Unlike many nations where healthcare emerged alongside, or directly from, broader social reform programs aimed at universal benefits, the American trajectory followed a markedly different path. The nation’s early development often prioritized individualism and limited government intervention, including in economic and social spheres. This inclination set the stage for a system where private enterprise, driven by profit motives, largely shaped the healthcare landscape. The laissez-faire principles gaining traction in the 19th and early 2leshoot century resonated with, and subsequently influenced, the structure of healthcare delivery, encouraging private investment and competition rather than immediate government intervention. This early preference for market-driven solutions over socialized ones created a fertile ground for the development of a capitalist healthcare framework.
Economic Foundations and Market Dynamics
Furthermore, the specific economic structure of the United States plays a colossal role. Its highly developed capitalistic system permeates all aspects of life, including health. Businesses, driven by market forces of supply and demand, investment returns, and competitive pressures, naturally gravitate towards healthcare as a significant spending area. This system incentivizes profit-making in health related services and products – from elective procedures demanding high-value pricing, to pharmaceuticals commanding vast profit margins, to diagnostic imaging requiring substantial capital investment. Businesses are fundamentally compelled to allocate resources where they perceive profitability. Consequently, the healthcare sector, in the US context, is vast and intricate, deeply integrated into a profit-driven economy. This dynamic creates an environment where market principles fundamentally shape access, cost, and the very nature of care provided.
The Paradox of Innovation and Cost
Undeniably, a persistent narrative praises the American system, particularly the portion dominated by private actors, for fostering groundbreaking biomedical research and technological innovations. Corporations invest heavily in research and development (R&D), leading to novel treatments, diagnostic tools, and therapeutic advancements without immediate public funding restrictions tied to specific outcomes or costs. This focus on maximizing returns on R&D investment often results in technological leadership across many medical fields. However, this very system operates on market principles, and like any commodity, healthcare services and technologies are auctioned to the highest bidder. As demand grows and the complexity of treatments increases, the costs escalate without a corresponding guarantee of wider accessibility outside of expensive insurance packages or direct payment. The high prices for innovation are not solely due to research costs; they are amplified by the lack of price regulation inherent in a capitalist system focused on market competition and shareholder value. This paradox where the system encourages innovation but demonstrably raises overall costs, often excluding vast segments without adequate coverage, is a core feature, not necessarily a flaw, of its capitalist architecture.
The Role of Financing and Employer-Based Insurance
This intricate system of financing is arguably its most distinctive characteristic – the near-universal linkage of health insurance to employment. In the US, the bulk of health insurance coverage comes not from individual mandates on the public dime or comprehensive national social insurance programs, but from private employers subsidizing (in whole or in part) the purchase of group health insurance plans for their employees. This structure is a direct outgrowth of tax policy decisions made decades ago, offering tax advantages to companies providing employee health benefits. It creates a massive market for standardized insurance plans, fostering an industry driven by competition among insurers and employers seeking to manage costs. While providing widespread access (in principle) and job security benefits, this financing model fundamentally ties healthcare to employment status. Consequently, job loss triggers a major disruption in coverage, creating vulnerability and contributing to precarious access even among employed populations. This employer-based model starkly contrasts with publicly financed systems where premiums or required contributions are tied to taxes, aiming for universal coverage regardless of employment status.
Culture, Values, and Political Will
Deep seated cultural and political factors significantly solidify and perpetuate this arrangement. The prevailing American emphasis on individual autonomy, personal responsibility, and skepticism towards centralized authority inherently clashes with the notion of a universally mandated, state-run healthcare system. The idea of the government directly providing healthcare is often viewed with suspicion, seen as an overreach of state power or a costly, inefficient failure. Conversely, systems in countries valuing social solidarity and community welfare emphasize collective responsibility, leading to political consensus and public acceptance for more government intervention, including direct funding of universal healthcare programs like social security or single-payer systems.
Furthermore, the political landscape in the US, highly polarized and often resistant to broad social reforms affecting healthcare funding and access, makes significant systemic change exceptionally difficult. The intricate web of powerful private lobbying groups, including major insurance companies, hospital systems, and pharmaceutical interests, exerts substantial influence, effectively countering efforts to implement universal public financing models or cap healthcare costs. These interests, well-funded and organized, successfully argue against intervention, reinforcing the status quo driven by market dynamics rather than public need.
Global Comparisons and Varying Destinations
Viewing this through a global lens reveals alternative, highly developed models achieving universal access without relying on a purely capitalist framework. Countries such as Canada, the United Kingdom, Germany, and Japan implement systems predominantly funded by general taxation or mandatory public insurance programs. These systems prioritize accessibility and equity, setting budgets, managing provider networks often contractually, and regulating costs to control spirals as seen in the US. While differing in specifics – Canada’s single-payer model, the UK’s National Health Service (NHS), Germany’s multi-payer system with sickness funds, Japan’s universal coverage funded by premiums and taxes – they share the core characteristic of publicly financed or heavily regulated universal healthcare. These systems demonstrate that a vastly different destination is possible under alternative financing and regulatory structures.
The Challenge of Affordability and Equity
Ergo, the question persists: why the divergent paths? The American model presents significant advantages in certain areas, notably in rapid innovation driven by corporate research investments. Yet, its disadvantages are equally profound – exorbitant costs, stark inequalities in access (with over 30 million currently uninsured), and complex, administratively burdensome systems. The challenge lies not just in understanding the *how*, but the *why*. What reinforces this historical trajectory in the 21st century? The undeniable fact is that despite occasional political pronouncements otherwise, the engine of the US healthcare system remains deeply entrenched in its capitalist, market-based origins. Changing this requires confronting deeply held cultural beliefs, overcoming formidable political resistance, and challenging the immense power of industry vested interests. Ignoring the vast, systemic cost escalation driven by profit motives and finite patient payers globally seems unlikely. Therefore, the US healthcare system is not merely an isolated anomaly; it represents a specific societal choice, perhaps the most commercially advanced nation on Earth still grappling with whether such advancement must be paid for primarily through the unfettered market forces or through collective, more regulated solutions.


